Postpartum Contraception
Fertility After Giving Birth
Predicting the return of fertility after giving birth is difficult and impacted by several factors, including breastfeeding.
- Some people will ovulate within 4 to 6 weeks of delivery.
- Ovulation returns before your menstrual period. For example, people ovulate and get a period 2 weeks later.
The return of fertility is unpredictable. Your doctor won’t be able to tell you when you are going to ovulate. Therefore, it is important for you to consider using contraception until you are ready to conceive again.
Common Misconceptions Among Postpartum People
I will not be interested in having sex during my postpartum period.
FALSE:
Libido in the postpartum period is variable, and there is no “normal.” After giving birth, libido is impacted by many things, including tissue healing, vaginal dryness related to low estrogen from breastfeeding and new demands of motherhood.
Contraception will negatively impact my ability to breastfeed.
FALSE:
There are several effective contraceptive methods that have no impact on breastfeeding or your baby.
If I am breastfeeding my baby, I don’t need to use birth control.
FALSE:
Breastfeeding is only effective at preventing pregnancy when you feed at least every 4 hours with no formula supplementation, for up to 6 months postpartum, assuming you haven’t gotten your period yet.
Choosing the Right Option for You
Factors to consider when choosing postpartum birth control include:
Hormonal vs. non-hormonal options:
Hormonal birth control comes in many forms (pill, patch, ring, injections, IUD) and may contain both estrogen and progesterone or progesterone alone. Estrogen-containing options may decrease breastmilk supply (see next page).
Reversible vs. permanent options:
Most birth control options are reversible. Reversible options do not delay the return of fertility when stopped. There are permanent forms of contraception for both men and women:
- Tubal sterilization (“Tubes tied”) for women
- Vasectomy for men
Other Considerations
Cost:
- Ranges from $0 to $400
- Many birth control options are covered by basic drug plans
- Ontario residents with OHIP coverage are eligible for free contraception when aged 25 years or younger
Effectiveness:
- 85 out of 100 women will get pregnant within one year without contraception
- If you are trying to prevent pregnancy in the postpartum period, it is important to have an effective and reliable form of birth control
- Methods range from 75% to >99% effectiveness
Route of administration:
- Having a newborn is a busy time. Different birth control options require different levels of attention. For example:
- Long-acting reversible contraception like the IUD or the progesterone implant need to be inserted by a health care provider, but typically require no attention after insertion
- Progesterone-only oral contraceptive pills must be taken everyday at the same time to prevent ovulation
If you have questions about what method of contraception is right for you during your postpartum period, you can ask your doctor or midwife. A postpartum visit typically happens 6 weeks after you have had your baby.
You can also find more information from the Society of Obstetricians and Gynaecologists of Canada (SOGC) about the post-partum period and birth control here: https://www.pregnancyinfo.ca/postpartum/postpartum/contraception/
Postpartum Contraception Decision Tree
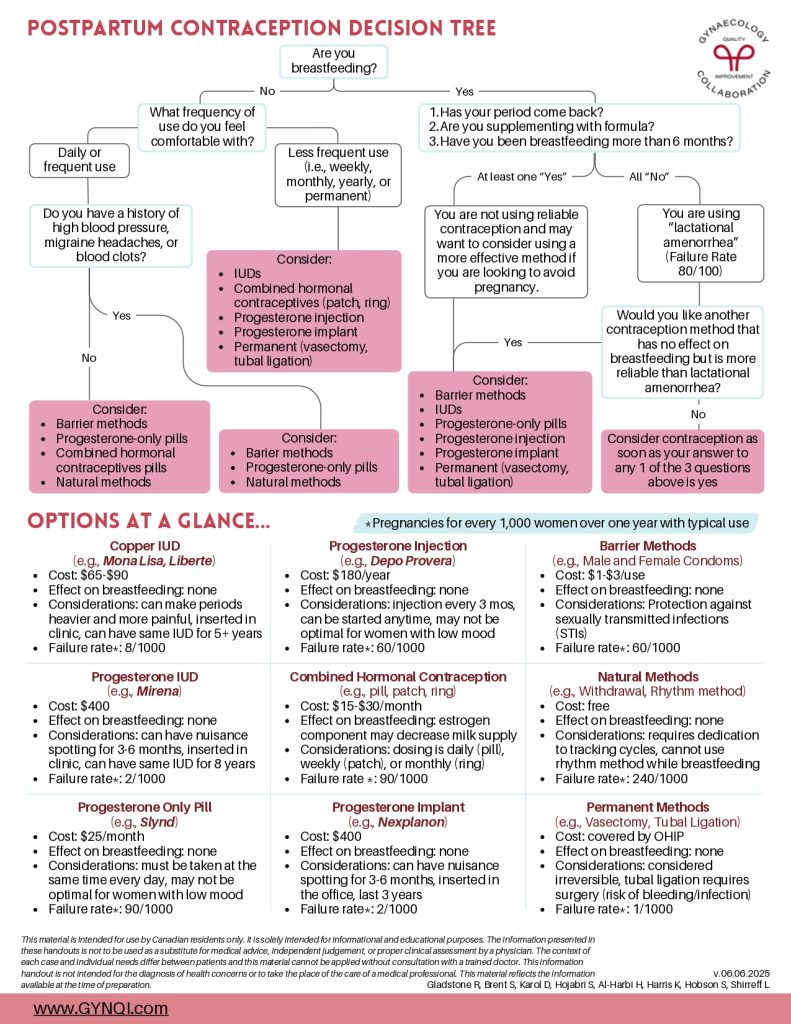
Are you breastfeeding?
- No: What frequency of use do you feel comfortable with?
- Daily or frequent use
- Do you have a history of high blood pressure, migraine headaches, or blood clots?
- No: consider
- Barrier methods
- Progesterone-only pills
- Combined hormonal contraceptives pills
- Natural methods
- Yes: consider
- Barrier methods
- Progesterone-only pills
- Natural methods
- No: consider
- Do you have a history of high blood pressure, migraine headaches, or blood clots?
- Less frequent use (i.e., weekly, monthly, yearly, or permanent): consider
- IUD
- Combined hormonal contraceptives (patch, ring)
- Progesterone injection
- Progesterone implant
- Permanent (vasectomy, tubal ligation)
- Daily or frequent use
- Yes: Has your period come back? Are you supplementing with formula? Have you been breastfeeding more than 6 months?
- At least one “Yes”
- You are not using reliable contraception and may want to consider using a more effective method if you are looking to avoid pregnancy. Consider:
- Barrier methods
- IUD
- Progesterone-only pills
- Progesterone injection
- Progesterone implant
- Permanent (vasectomy, tubal ligation)
- You are not using reliable contraception and may want to consider using a more effective method if you are looking to avoid pregnancy. Consider:
- All “No”
- You are using “lactational amenorrhea” (Failure Rate 80/100)
- Would you like another contraception method that has no effect on breastfeeding but is more reliable than lactational amenorrhea?
- Yes: consider
- Barrier methods
- IUDs
- Progesterone-only pills
- Progesterone injection
- Progesterone implant
- Permanent (vasectomy, tubal ligation)
- No: consider contraception as soon as your answer to any 1 of the 3 questions above is yes
- Yes: consider
- Would you like another contraception method that has no effect on breastfeeding but is more reliable than lactational amenorrhea?
- You are using “lactational amenorrhea” (Failure Rate 80/100)
- At least one “Yes”
Options At A Glance…
*Pregnancies for every 1,000 women over one year with typical use
Copper IUD (e.g., Mona Lisa, Liberte)
- Cost: $65-$90
- Effect on breastfeeding: none
- Considerations: can make periods heavier and more painful, inserted in clinic, can have same IUD for 5+ years
- Failure rate*: 8/1000
Progesterone IUD (e.g., Mirena)
- Cost: $400
- Effect on breastfeeding: none
- Considerations: can have nuisance spotting for 3-6 months, inserted in clinic, can have same IUD for 8 years
- Failure rate*: 2/1000
Progesterone Only Pill (e.g., Slynd)
- Cost: $25/month
- Effect on breastfeeding: none
- Considerations: must be taken at the same time every day, may not be optimal for women with low mood
- Failure rate*: 90/1000
Progesterone Injection (e.g., Depo Provera)
- Cost: $180/year
- Effect on breastfeeding: none
- Considerations: injection every 3 mos, can be started anytime, may not be optimal for women with low mood
- Failure rate*: 60/1000
Combined Hormonal Contraception (e.g., pill, patch, ring)
- Cost: $15-$30/month
- Effect on breastfeeding: estrogen component may decrease milk supply
- Considerations: dosing is daily (pill), weekly (patch), or monthly (ring)
- Failure rate *: 90/1000
Progesterone Implant (e.g., Nexplanon)
- Cost: $400
- Effect on breastfeeding: none
- Considerations: can have nuisance spotting for 3-6 months, inserted in the office, last 3 years
- Failure rate*: 2/1000
Barrier Methods (e.g., Male and Female Condoms)
- Cost: $1-$3/use
- Effect on breastfeeding: none
- Considerations: Protection against sexually transmitted infections (STIs)
- Failure rate*: 60/1000
Natural Methods (e.g., Withdrawal Rhythm Method)
- Cost: free
- Effect on breastfeeding: none
- Considerations: requires dedication to tracking cycles, cannot use rhythm method while breastfeeding
- Failure rate*: 240/1000
Permanent Methods (e.g., Vasectomy, Tubal Ligation)
- Cost: covered by OHIP
- Effect on breastfeeding: none
- Considerations: considered irreversible, tubal ligation requires surgery (risk of bleeding/infection)
- Failure rate*: 1/1000


